Over the next bit, I am going to be digging into a presentation by Dr. Jeffrey Weber - see it for yourself here: Immunotherapy for cancer: the journey so far, and where are we headed? Cancer Crosslinks 2018
With so many Stage III melanoma patients now gaining access to adjuvant care and all the inherent questions pertinent to that, combined with the fact that adjuvant treatment is what I attained for my melanoma journey, albeit as a Stage IV patient, I will start there. Before we get into the weeds, here is an overview of current approved therapies for melanoma I wrote in 2017 that sadly, other than a change in dosing options for the administration of Opdivo, has not needed any significant updates since: Melanoma Intel: A primer for current standard of care and treatment options
Here is an article that does pretty much the same thing, written in 2018: Melanoma treatment in review
LATE ADDENDUM: FINALLY!!!! There was reason to update the primer - April 2022 - Primer for Current Melanoma Treatments - New and Improved Version 2022!!!!
I recently penned some information for a Stage III patient dealing with the confusion that a melanoma diagnosis and adjuvant treatment can engender, and it seems a pretty good place to start:
It is very easy to get confused with all the "data" floating around. Numbers repeated in the media (as opposed to medical literature) and unfortunately even occasionally tossed around in doctor's offices without clear explanation can create more confusion than clarity. One of those oft quoted bits is the "50% survival rate" of melanoma patients vs various low rates from 10-20-something % that "melanoma patients used to have". All of this can get confusing really quickly because you have to make sure you are talking about the right drug, used in folks in the stage you are discussing AND the right category of "response". Are the studies describing "response rate", "progression free response", "overall survival", or what?????? Those categories can mean very different things. Further, I've seen lots of patients misunderstand the significance of the FDA approval dates for both targeted and immunotherapy as ADJUVANT vs the date of their approval for melanoma overall.
Here's a little breakdown of FDA approval dates:
The first targeted therapy for BRAF positive melanoma patients was approved in 2011. Targeted therapy for adjuvant use in melanoma was approved in 2018.
The first effective immunotherapy with its 15% response rate in Stage IV melanoma was ipilimumab (Yervoy - an anti-CTLA-4 product) ~ approved in 2011. Its approval for use as adjuvant was in 2015.
Anti-PD-1 immunotherapy products, Nivolumab (Opdivo) and Pembrolizumab (Keytruda) were approved for unresectable/Stage IV melanoma in 2014. Both have roughly a 40% response rate in those patients with a similar side effect profile that is less severe than that of ipi. Opdivo was approved in combination with ipi for metastatic patients in 2015. That combo is currently in trials as adjuvant. Opdivo was approved for use as adjuvant in melanoma patients in 2017. Keytruda was approved for adjuvant use in Stage III patients 2019. {LATE NOTE: Keytruda was also approved for Stage II patients in 2021.}
As a person who was likely somewhere between the 28th - 36th person in the United States to take nivolumab, via a clinical trial in the ADJUVANT arm as a Stage IV melanoma patient in 2010!!!!!!!!!!!! - I know from experience that it makes a HUGE difference in having a collection of data and information behind your treatment option and NOT!!!! Here's a little story that tells the history of Opdivo or as I took it - MDX-1106 - if you are interested: Love Potion...or Patient...#9!!!!!
The date of FDA approval for use in melanoma patients generally matters - even to those who are using it as adjuvant today. In the case of Opdivo, it means that under FDA approval (apart from the fact that melanoma ratties in the United States had been taking Opdivo since 2009) melanoma patients were treated with Opdivo since 2014. Studies from us ratties as well as data that grew with the 2014 approval consistently show that folks with Stage III and Stage IV inoperable melanoma have response rates of around 40% when Opdivo is used as a single agent and through that use we learned what dosage to administer, the likely side effects, rare adverse events that might be encountered, how long they last, and how best to treat them. Important information that you do not have when a drug is first being used to treat a particular disease.
In all that trial and error - ie learning - researchers discovered that folks with melanoma responded best to immunotherapy when they had the least possible disease burden. This leads us to adjuvant therapy. Adjuvant therapy is given to a person when their tumor has been removed by surgery and/or radiation. Despite knowing since my trial - though the data wasn't published until 2014 - that we 33 ratties (2 stage IIIC and 31 Stage IV ) did very well when we took Opdivo as adjuvant, the FDA did not see fit to approve Opdivo for adjuvant use in melanoma until 2017. You can see the results of the adjuvant arm of my study here: C'est moi!!! Results from the 33 ratties in my Nivolumb/Opdivo trial...published!
It notes: "Our data suggest that nivo is clinically active in resected stage IIIC/IV melanoma, based on low rate of relapse (10 of 33), impressive relapse-free survival - estimated RFS of 47.1 months, and median overall survival not yet reached with over 32 months of follow up." REMEMBER - we have learned even more since then!!!!!!!!!!!!!!!!!!!!
Here is a report on ipi vs nivo in the adjuvant melanoma setting from 2017: Nivo better than ipi as adjuvant treatment for melanoma! Surprise, surprise, surprise!!!
That study shows ~ Recurrence free survival at 18 months: 66.4% for nivo 52.7% for ipi
OVERALL recurrence free survival was 70.5% for the nivo group (vs 60.8% for ipi) at 1 year...but...when you pull out the Stage IV folks the number was 63% for nivo vs only 57% for ipi.
OVERALL recurrence free survival was 70.5% for the nivo group (vs 60.8% for ipi) at 1 year...but...when you pull out the Stage IV folks the number was 63% for nivo vs only 57% for ipi.
NOW! When you break things down further, as the info above is beginning to show, folks who are Stage III do better than folks who are Stage IV no matter what you do or don't do to them. So you can't just take all the information gleaned from Stage IV patients and throw it at Stage III patients as fact. For instance, in the last report in this post from 2019, that addresses Stage III melanoma patients treated with Yervoy (which we already KNOW from the other report does NOT work as well for melanoma patients whether Stage III or Stage IV when used as a single agent compared to anti-PD-1) vs placebo noted in this link: I've said it before, I'll say it again - ENOUGH ALREADY! No more interferon for melanoma!!! (Or placebos - for that matter!!!) You will see that Stage III melanoma patients, even treated only with ipi, had an "overall survival rate of 60% at 7 years". To be fair the placebo group had an OS of 51.3%. Hell, even I lived as a Stage IIIB melanoma patient for 7 years with no treatment beyond surgery before advancing to Stage IV and am still here after brain and lung mets and my nivo trial and remain NED for melanoma.
Bottom line - comparing apples to apples matters. The amount we have learned about anti-PD-1 since melanoma ratties started taking it in the States in 2009 and after it gained FDA approval for use in melanoma patients in 2014 makes a world of difference to all of us.
Now for the report from Dr. Weber, which begins with a review of immunotherapy for melanoma generally:









And with that history, we begin to explore immunotherapy as adjuvant for melanoma -







 |
| Yep - this was me and my fellow ratties. I was in Cohort 1. |

This data justified a trial of adjuvant nivolizumab versus standard ipilimumab -








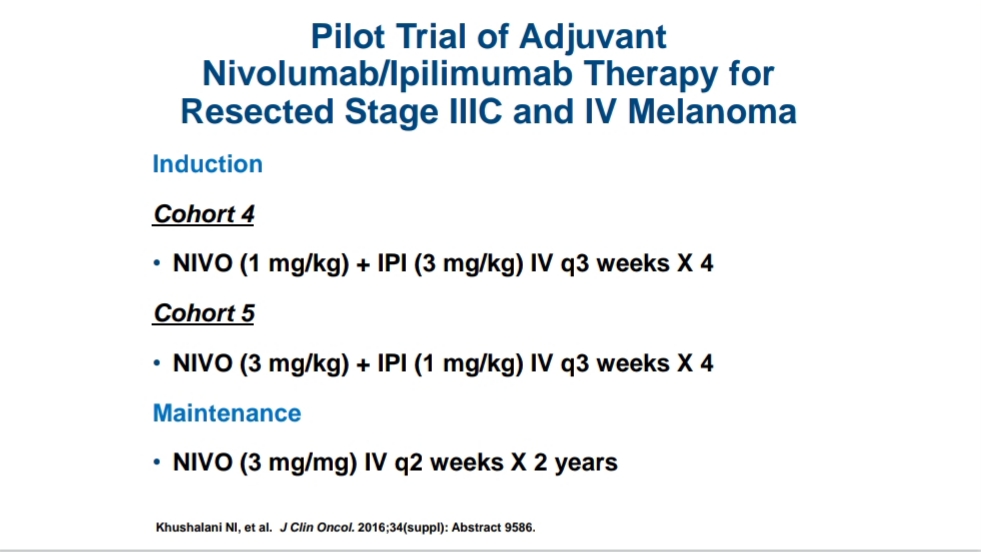
NEXT - pilot nivo with ipi data justified a new adjuvant trial of nivo + ipi vs nivo with new biomarkers -


Forgive the blurry slides I've reproduced here. Check the link at the top to view them for yourselves. Hope this helps. We've come a long way, though we have further to go. Coming soon - the furture of immunotherapy for cancer....
Ratties rock! - c





